Sleep apnea means that your breathing often is blocked or partly blocked during sleep. The problem can be mild to severe, based on how often your lungs don’t get enough air. This may happen from 5 to more than 50 times an hour.
This topic focuses on obstructive sleep apnea, which is the most common type.
A less common type of apnea called central sleep apnea can occur in people who have had a stroke, have heart failure, or have a brain tumor or infection. Even though this topic isn’t about central sleep apnea, some of the treatments discussed here may also help treat it. Talk with your doctor to find out more about central sleep apnea.
What causes obstructive sleep apnea?
Blocked or narrowed airways in your nose, mouth, or throat can cause sleep apnea. Your airways can become blocked when your throat muscles and tongue relax during sleep.
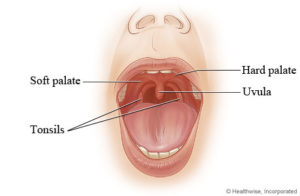
Sleep apnea can also occur if you have large tonsils or adenoids. During the day, when you are awake and standing up, these may not cause problems. But when you lie down at night, they can press down on your airway, narrowing it and causing sleep apnea. Sleep apnea can also occur if you have a problem with your jawbone.
In children, the main cause of sleep apnea is large tonsils or adenoids.
Sleep apnea is more likely to occur if you are overweight, use certain medicines or alcohol before bed, or sleep on your back.
What are the symptoms?
The main symptoms of sleep apnea that you may notice are:
- Not feeling rested after a night’s sleep.
- Feeling sleepy during the day.
- Waking up with a headache.
Your bed partner may notice that while you sleep:
- You stop breathing.
- You often snore loudly.
- You gasp or choke.
- You toss and turn.
Children who have sleep apnea:
- Nearly always snores.
- May be hyperactive or have problems paying attention during the day.
- May be restless during sleep and wake up often. They also may have problems with bed-wetting.
But children may not seem very sleepy during the day (a key symptom in adults). The only symptom of sleep apnea in some children may be that they do not grow as quickly as most children their age.
Can sleep apnea cause other problems?
Having sleep apnea can lead to serious problems such as:
- High blood pressure.
- High blood pressure in your lungs.
- An abnormal heart rhythm, heart failure, coronary artery disease (CAD), or stroke.
- Depression.
- Diabetes.
If you have sleep apnea, you also may not be sleeping as well as you could. If you feel sleepy during the day and this gets in the way of the normal things you do (like work, school, or driving), it’s important to talk to your doctor. Be safe. Do not drive while you are drowsy.
How is sleep apnea diagnosed?
Your doctor will probably examine you and ask about your past health. He or she may also ask you or your sleep partner about your snoring and sleep behavior and how tired you feel during the day.
Your doctor may suggest a sleep study. A sleep study usually takes place at a sleep center, where you will spend the night. Sleep studies find out how often you stop breathing or have too little air flowing into your lungs during sleep. They also find out how much oxygen you have in your blood during sleep. You may have blood tests and X-rays.
How is it treated?
You may be able to treat mild sleep apnea by making changes in how you live and the way you sleep. For example:
- Lose weight if you are overweight.
- Sleep on your side and not your back.
- Avoid alcohol and medicines such as sedatives before bed.
If lifestyle changes don’t help sleep apnea, you may be able to use an oral breathing device or other types of devices. These devices help keep your airways open while you sleep.
Sleep apnea is often treated with a machine that helps you breathe while you sleep. This treatment is called continuous positive airway pressure, or CPAP (say “SEE-pap”). Sometimes medicine that helps you stay awake during the day may be used along with CPAP. If your tonsils, adenoids, uvula, or other tissues are blocking your airway, your doctor may suggest surgery to open your airway.